My favorite line is "anything that would not turn up in an autopsy, as in depression or agoraphobia, cannot be equated with physical illness". Much of what we do won't show up on an autopsy! Heart arrythymias, seizures, even a potassium chloride overdose won't show up on autopsy. These false dichotomies have got to go.
Monday, March 31, 2008
Mental Health Parity
Interesting article in the New York Times this weekend. Click here to read it. It is fascinating to me that there are still people in the world who value physical illness differently than mental illness. Why? We can't prevent a heart attack by "force of will". Why do we insist that, if the brain goes haywire, it is fixable with just a bit more attention to detail. Why is a feeling of soreness in the throat more valid than the a feeling of hopelessness? What can we be exhausted from the flu but not post-partum depression. I know that those of you in practice know what I am talking about.
Crisis Teams: When does a crisis involve boots on the ground?
Families are frustrated by long waits in the Psychiatric Emergency Rooms that are happening all over the Commonwealth, and the remedy proposed that we move those services out to the home. One would hope that, in the context of Intense Care Coordination and consistent screening programs, we would have fewer families in crisis requiring that level of intervention. Crisis intervention is a terrible way to manage mental illness. Of course, it will be difficult to maintain a level of expertise in this area as it becomes less common.
(1) What suggestions do you have for structuring the Mobile Crisis Intervention service across the Commonwealth?
(2) What is the appropriate number and qualifications of staff for a Mobile Crisis Intervention team?
(1) What suggestions do you have for structuring the Mobile Crisis Intervention service across the Commonwealth?
The first thing to realize is that a 45 minute response time is not possible in many parts of the Commonwealth unless Masshealth is going to pay for helicopters. In South Worcester County, it takes that long to get to Brimfield or Ware. The standards for “Crisis intervention” need to be rewritten to reflect that reality. Most crises happen in the context of poorly coordinated care for children previously identified as having difficulty. That said, crisis management requires three things:
1) “De-escalation”: Like Henry Goldblum on the old “Hill St. Blues” TV show, we need people among the “first responders” (police, EMT and fire fighters) who are able to “talk down” the person involved in the “immediately” dangerous behavior. That person should be local, and able to contact the Mobile Crisis Team for the region in which they work.
2) Transporation protocols: Universal protocols for transport to Emergency Mental Health Services, covering issues such as the use of physical and chemical restraint, ambulances vs. police vehicles and notification of family.
3) Mobile Crisis Protocols: These should include discretionary powers on behalf of the Team to decide the level of intervention needed at this time.
4) Emergency Planning: Calling the team or designation as a member of the SED class should involve the development of an individualized emergency plan for the child and family.
1) “De-escalation”: Like Henry Goldblum on the old “Hill St. Blues” TV show, we need people among the “first responders” (police, EMT and fire fighters) who are able to “talk down” the person involved in the “immediately” dangerous behavior. That person should be local, and able to contact the Mobile Crisis Team for the region in which they work.
2) Transporation protocols: Universal protocols for transport to Emergency Mental Health Services, covering issues such as the use of physical and chemical restraint, ambulances vs. police vehicles and notification of family.
3) Mobile Crisis Protocols: These should include discretionary powers on behalf of the Team to decide the level of intervention needed at this time.
4) Emergency Planning: Calling the team or designation as a member of the SED class should involve the development of an individualized emergency plan for the child and family.
(2) What is the appropriate number and qualifications of staff for a Mobile Crisis Intervention team?
They probably need to be similar to the requirement for Emergency Mental Health work in general.
(3)What suggestions do you have regarding coordination of Mobile Crisis Intervention with other services, including the other Initiative Services discussed in this RFI?
(3)What suggestions do you have regarding coordination of Mobile Crisis Intervention with other services, including the other Initiative Services discussed in this RFI?
From Chris Stille:
As discussed in the response to 2.1.3, 2.3.B(1) and 2.3.B(4), there is a need for crisis plans and crisis teams to engage in communication and coordination with the child's ongoing medical (including primary care) and mental health service providers, as well as with their school. The goal of this process would be to help children and families transition smoothly between levels of care (both up and down the urgency/intensiveness ladder). We feel this would be facilitated by proactive designation of a person or small group of people as each child's crisis team, ideally determined BEFORE a crisis occurs. This would further enable well-planned, well-coordinated care.
Amen.
Wednesday, March 26, 2008
Collaboration: The friend of Rosie D.
The meat of the matter- how do we collaborate? Most of the children in the class of SED were buffeted about the system like the kid in "Officer Krupke" from "West Side Story". How do we break through the silos? How do we make it all come together?
(1) What structure(s) would best support collaborative practice between public agencies and among private providers? What are the advantages and disadvantages of addressing coordination issues among public agencies and private provider agencies in the same forum? Should there be separate settings for these discussions? How can MassHealth best ensure integration of all aspects of delivery of care and mutual accountability for outcomes?
(2) What are your suggestions for ensuring collaborative practice among different individual providers or provider agencies serving the same child/family?
(3) What are your suggestions for SOC Committee membership and meeting format to balance the value of having family and youth represented on the Committee with the need to protect the privacy of children and families involved in ICC?
(4) What are the advantages and disadvantages of combining discussions of policy and general coordination with discussions of specific service coordination problems, which would require disclosing personal information? Should there be separate settings for these discussions?
(5) What suggestions do you have or lessons have you learned for facilitating partnerships with school districts?
In general, all agencies have a specific mission, and they will collaborate with “outsiders” based on the abilitiy of the outsider to help them to achieve that mission. With schools, it is about improving educational outcome, so as an “outsider”, I have had to think about how my expertise can help a school system accomplish its mission (and how they can help me to accomplish mine). This is a nuanced take on the prime question “How can I help this child”. Several other hints:
1) Show up. Schools respond to people to respond to them through team meetings.
2) Match objectives: Completing homework is a great measurable behavioral objective that meets my needs as a prescriber and their needs as educators.
3) Share information: A five minute phone discussion can cut through weeks of written messages.
4) Understand their schedule: Schools are open on school days and are generally closed by 3 PM. Call in the morning.
(6) What suggestions do you have or lessons have you learned for facilitating partnerships with juvenile courts? Probation?
(7) What suggestions do you have or lessons have you learned for facilitating partnerships with broader system partners?
(8) Do you have any other comments or suggestions on these subjects?
(1) What structure(s) would best support collaborative practice between public agencies and among private providers? What are the advantages and disadvantages of addressing coordination issues among public agencies and private provider agencies in the same forum? Should there be separate settings for these discussions? How can MassHealth best ensure integration of all aspects of delivery of care and mutual accountability for outcomes?
This is a tricky question, and key to the outcomes of this remedy. The structure that will best support collaborative practice is the one that best allows integration of the needs and strengths of the family with abilities and resources of the agencies involved. The ICC will need to work with the family in the process of developing the service plan to identify the structure that will support the family best, and assure that the agencies and providers are able to utilize that format. At some level, it is important to put faces to words, but much of the work can likely be accomplished through virtual formats. MassHealth needs to ensure that there is regular communication within the treatment team, to avoid a crisis-focused approach.
MassHealth should provide for a variety of formats to accomodate the different types of teams with which we are dealing:
1) Face-to-face: Catalog and contact information for facilities willing to host multidisciplinary team meetings, travel reimbursement, access to on-line scheduling service.
2) Phone meeting: Reimbursement to support time and cost of conference calls.
3) Virtual meetings: Secure "chat rooms" and "bulletin boards" for sharing confidential informantion.
4) Shared single care plan: On-line care plan accessible to all parties (so that each can see what the other is doing).
It seems likely that an initial "face-to-face" meeting followed by routine conference calls will likely be the preferred format for interaction, but, ultimately, the adequacy of the interaction should be judged by the needs of the family and the outcomes of care.
(2) What are your suggestions for ensuring collaborative practice among different individual providers or provider agencies serving the same child/family?
The current system of reimbursement does not encourage collaborative behavior- the various components of the system are rewarded for each piece of work done, not for work avoided through collaboration. Reimbursement needs to reflect the quality of the interaction as well as the quantity of the services provided. I would suggest considering the families assessment of the degree of collaboration as a multiplier to reward collaborative behavior.
(3) What are your suggestions for SOC Committee membership and meeting format to balance the value of having family and youth represented on the Committee with the need to protect the privacy of children and families involved in ICC?
In a truly family-centered paradigm, it is difficult to imagine “one size fitting all”; the SOC membership needs to reflect the array of services and service providers that are working with a given family. This is a deeply personal negations between the intensive care coordinator and the family. Some portions are non-negotiable (ie. DSS must be involved with clients engaged in the system, whether the family wants it or not) and it will be difficult when the family has had conflict with one of the agencies essential to service delivery (ie if the family has long-standing disputes with the Special Education Department, they may not want to invite them to be on the team even though they are essential to the process). I suspect that the most difficult cases will be those in which custody is in dispute. The care coordinator needs to be given discretion and training to negotiate and sometime mandate who will be on the team.
(4) What are the advantages and disadvantages of combining discussions of policy and general coordination with discussions of specific service coordination problems, which would require disclosing personal information? Should there be separate settings for these discussions?
Generally, these discussions take place at different levels within agencies. While it is important for fieldwork to inform policy, field workers are usually not in a position to set policy, except in some of the smaller agencies. Still, in order to relate policy to reality, it is important to have discussions in which those that set policy hear how the policy plays out in specific cases. In medical culture, this occurs at the “M and M” conference, in which the details of a specific case are discussed (with identifiers removcd) in a secure and non-discoverable environment (papers burned afterwards). This may be a model that would be useful to this process of multi-agency collaboration, and may require legislative protection similar to that afforded medical staff in hospitals.
(5) What suggestions do you have or lessons have you learned for facilitating partnerships with school districts?
In general, all agencies have a specific mission, and they will collaborate with “outsiders” based on the abilitiy of the outsider to help them to achieve that mission. With schools, it is about improving educational outcome, so as an “outsider”, I have had to think about how my expertise can help a school system accomplish its mission (and how they can help me to accomplish mine). This is a nuanced take on the prime question “How can I help this child”. Several other hints:
1) Show up. Schools respond to people to respond to them through team meetings.
2) Match objectives: Completing homework is a great measurable behavioral objective that meets my needs as a prescriber and their needs as educators.
3) Share information: A five minute phone discussion can cut through weeks of written messages.
4) Understand their schedule: Schools are open on school days and are generally closed by 3 PM. Call in the morning.
(6) What suggestions do you have or lessons have you learned for facilitating partnerships with juvenile courts? Probation?
Actually, substitute courts and probabtion for schools in the above paragraph, and you have a reasonable set of advice.
(7) What suggestions do you have or lessons have you learned for facilitating partnerships with broader system partners?
Ditto.
(8) Do you have any other comments or suggestions on these subjects?
All of this collaboration takes time, and we need to reimburse individuals and agencies for taking the time to collaborate.
Guest Spot: Disabilities Sensitivity is a Cultural Competence
I am writing in this blog to advocate one component of cultural competence. I am aware that there are some organizations in the Boston area who are hired to train mental health professionals and social service workers on multicultural sensitivity training. I attended one such training last year and though the information and presentation was excellent by "Families First," it did not provide any information on how to work with individuals with disabilities.
Mass Health can implement Disability sensitivity as one component of Cultural Competence. By coincidence, Blue Cross/Blue Shield of Massachusetts interviewed me two weeks ago about the need to include the above topic as a cultural competence for mental health professionals. It is also important that medical professionals also receive the same training in this area as well. Currently, Tufts University and I believe UMASS has patient-doctor trainings in which "hired" patients train doctors on how to interact with them and to understand their symptoms. I heard positive feedback from persons with disabilities who participate as patients in this training.
Mass Health can recommend that clinics/facilities that staff receive trainings similar to the Patient/Doctor model that is currently being used. The question is how to pay staff to attend such trainings. That is always the tricky part of the equation. For mental health professionals, CEUs can be awarded to going a training during a staff meeting or a special meeting time. But again, mental health clinicians do not get paid for mandated staff meetings. This issue of payment or compensation has to worked between Mass Health and the provider.
Why do medical and mental health professionals need to learn to be more culturally competent in this area?
1) The is a new population of veterans coming home from Iraq and Afganhistan who are newly disabled and will need both medical and mental health services. The current health insurance benefit for vets is not adequate to cover all their healthcare needs.
2) More and more persons with disabilities across the board are living in the community and not necessarily in institutions. Governor Patrick's plan for Long Term call for more funding to be used for community based services for individuals with psychiatric disabilities; developmental disabilities with physical disabilities to live in the community across the commonwealth.
3) Professionally and personally speaking, I heard numerous complaints from consumers and advocates with disabilities vent their frustrations on how their medical or mental health professional treated them for their symptoms. An example is when an individual goes to a health facility with a personal care attendant, the medical professional tends to talk to the PCA and not to the client. Another example is when a colleague of mine who is a wheelchair user told me how her mental health clinician told her to go fight her "revolution" during the last session. The revolution is about the barriers in the environment that prevent persons with disabilities from enjoying the same freedoms as their able-bodied counterparts. We both wondered if she would tell a person from a multicultural background the same information. I think not..
Robbin Miller
Advocate/Counselor
Mass Health can implement Disability sensitivity as one component of Cultural Competence. By coincidence, Blue Cross/Blue Shield of Massachusetts interviewed me two weeks ago about the need to include the above topic as a cultural competence for mental health professionals. It is also important that medical professionals also receive the same training in this area as well. Currently, Tufts University and I believe UMASS has patient-doctor trainings in which "hired" patients train doctors on how to interact with them and to understand their symptoms. I heard positive feedback from persons with disabilities who participate as patients in this training.
Mass Health can recommend that clinics/facilities that staff receive trainings similar to the Patient/Doctor model that is currently being used. The question is how to pay staff to attend such trainings. That is always the tricky part of the equation. For mental health professionals, CEUs can be awarded to going a training during a staff meeting or a special meeting time. But again, mental health clinicians do not get paid for mandated staff meetings. This issue of payment or compensation has to worked between Mass Health and the provider.
Why do medical and mental health professionals need to learn to be more culturally competent in this area?
1) The is a new population of veterans coming home from Iraq and Afganhistan who are newly disabled and will need both medical and mental health services. The current health insurance benefit for vets is not adequate to cover all their healthcare needs.
2) More and more persons with disabilities across the board are living in the community and not necessarily in institutions. Governor Patrick's plan for Long Term call for more funding to be used for community based services for individuals with psychiatric disabilities; developmental disabilities with physical disabilities to live in the community across the commonwealth.
3) Professionally and personally speaking, I heard numerous complaints from consumers and advocates with disabilities vent their frustrations on how their medical or mental health professional treated them for their symptoms. An example is when an individual goes to a health facility with a personal care attendant, the medical professional tends to talk to the PCA and not to the client. Another example is when a colleague of mine who is a wheelchair user told me how her mental health clinician told her to go fight her "revolution" during the last session. The revolution is about the barriers in the environment that prevent persons with disabilities from enjoying the same freedoms as their able-bodied counterparts. We both wondered if she would tell a person from a multicultural background the same information. I think not..
Robbin Miller
Advocate/Counselor
The Culture Question: What is the culture of the Commonwealth?
I have been getting feedback from many of you in the Network. Thank you. I have elected to not edit my draft responses on the blog, but to integrate your comments into the "final document", which I will try to post as a .pdf next week. We will see how this goes.
This is an incredibly challenging issue, as we are facing an array of patients from a variety of backgrounds like we have never seen before. A few ideas:
-----------------------------------------------------------------------------------------
These are hard questions.
(1) CSAs will serve relatively large areas with diverse populations. It may be difficult for one organization to have the cultural expertise to effectively serve such a broad range of needs. What strategies would you suggest to ensure that culturally competent care is available for all MassHealth children and families who need behavioral health services in a given Service Area?This is an incredibly challenging issue, as we are facing an array of patients from a variety of backgrounds like we have never seen before. A few ideas:
1) Development of a statewide registry of resources (people) and services provided throughout the Commonwealth. This would allow interagency referral and facilitate the ability of people to address needs when there are no local resources.
2) Adequately funding the use of "off-site" interpreters for folks with language needs that cannot be met locally. This requires providers to have the proper equipment (ie. speakphones or videoconferencing capability in the exam rooms)
3) Developing a "fast track" to recruit and credential therapists who were born and raised in other cultures. They may help to provide some level of service.
4) Support agencies that recognize their limitations and seek outside support, rather than penalize them for not having the right services on-site.
(2) What suggestions do you have for strategies to reduce any health care disparities in the area of behavioral health?
First and foremost, we need to track the screening and referrals of folks with respect to race and ethnicity, so that we can actually get a handle on what the disparities are. It is sometimes challenging to assign patients to a certain race and ethnicity, and one certainly difficult to deal with a problem until you have defined it. We should also engage in a discussion (or perhaps focus groups) to identify barriers perceived by different sub-populations and respond to them. Finally, we need to push the definition of patient focused care to incorporate the families health belief system into the treatment plan. I defer to the group regarding other ideas.
First and foremost, we need to track the screening and referrals of folks with respect to race and ethnicity, so that we can actually get a handle on what the disparities are. It is sometimes challenging to assign patients to a certain race and ethnicity, and one certainly difficult to deal with a problem until you have defined it. We should also engage in a discussion (or perhaps focus groups) to identify barriers perceived by different sub-populations and respond to them. Finally, we need to push the definition of patient focused care to incorporate the families health belief system into the treatment plan. I defer to the group regarding other ideas.
(3) Are there models of culturally competent care you think MassHealth should consider?
Yes. One is the the "Latino Mental Health Project, which partners the Massachusetts Department of Mental Health with community health centers and local health care providers to identify barriers preventing Latinos from seeking mental health care. With a grant from the American Psychiatric Foundation, CMAHEC created “Hablemos en Familia,” a series of workshops educating Latino community members to recognize, cope with and seek treatment. The federal Office of Minority Health recognized the program and selected CMAHEC from 500 entries to present at its national leadership summit.".
Another is the HOPE Coalition (Healthy Options for Prevention and Education) is a youth-adult partnership coalition created to reduce youth violence, substance use and promote adolescent mental health in the City of Worcester. (Laurie Ross, Coordinator Phone: (508) 793-7642 , Email: LRoss@clarku.edu). Both of these build on partnerships with community-based organizations to make it all work.
Monday, March 24, 2008
CSAs: What are they good for?
Now we are getting to the heart of the Rosie D remedy: the CSA. According to the guidance:
"... the CSA will provide ICC to MassHealth-enrolled children and youth in the Service Area. ICC will provide the Wraparound Care Planning model of care coordination. Wraparound Care Planning is based on an ecological understanding of the child and the child’s functioning. The process assesses, engages, and works with all aspects of the child’s “ecology”: the child’s physical and mental health, family, extended family, peers, school, recreation, and communities to which s/he belongs. To effectively partner with families to engage this full breadth of the child’s world, the CSA needs to have and continually nurture relationships throughout its community, including with primary care providers, hospitals, schools, community agencies, other providers, recreational programs, child care resources, housing and food programs, residential and shelter providers.
The CSA also needs to be able to train, supervise and administratively support the clinical and paraprofessional staff who will be working with children and families in ICC. The Wraparound Care Planning model is promising in its ability to develop highly individualized, clinically sophisticated, multi-dimensional care plans. However, for the very same reasons, it is a challenging model to learn, to master and to sustain."
Good point. It needs to be addressed openly. You will need to demonstrate a firewall between the "care-coordination" side of things and the service delivery side.
"... the CSA will provide ICC to MassHealth-enrolled children and youth in the Service Area. ICC will provide the Wraparound Care Planning model of care coordination. Wraparound Care Planning is based on an ecological understanding of the child and the child’s functioning. The process assesses, engages, and works with all aspects of the child’s “ecology”: the child’s physical and mental health, family, extended family, peers, school, recreation, and communities to which s/he belongs. To effectively partner with families to engage this full breadth of the child’s world, the CSA needs to have and continually nurture relationships throughout its community, including with primary care providers, hospitals, schools, community agencies, other providers, recreational programs, child care resources, housing and food programs, residential and shelter providers.
The CSA also needs to be able to train, supervise and administratively support the clinical and paraprofessional staff who will be working with children and families in ICC. The Wraparound Care Planning model is promising in its ability to develop highly individualized, clinically sophisticated, multi-dimensional care plans. However, for the very same reasons, it is a challenging model to learn, to master and to sustain."
These CSAs sound like a cross between Annie Sullivan, Saul Alinsky and Jane Addams. Can this really be done? Anyway, the RFI looks for our input.
(1) Do you have any comments or suggestions on the proposed CSA qualifications?
(1) Do you have any comments or suggestions on the proposed CSA qualifications?
My first comment is one of wonder; the bar is set (appropriately) quite high for this program, and it is not clear to me who will achieve that standard. I am concerned about that the need to provide services from birth to 21 will restrict the ability of some agencies to apply, as the needs of families vary so much over that time span. I am also concerned about having in place a model of Wraparound Services. I suspect that, in many parts of the state, these CSAs will be "start-ups" because noone is doing Wraparound at present.
(2) How do you suggest addressing potential conflicts of interest for ICC providers who self-refer?
Sunday, March 23, 2008
More questions. Ever more questions.
More questions from the RFI:
(1) How should CSAs ensure that Care Planning Teams have access to needed medical and psychiatric expertise?
(3) Based on your program experience and knowledge of the clinical workforce issues in your region of Massachusetts, what staffing arrangements make most sense for CSAs in providing medical and psychiatric expertise? Which disciplines (e.g., child psychiatrist, child-trained APRN, child-trained RN, behavioral pediatrician, or other medical professionals) can be most useful in which roles?
(4) What suggestions/lessons learned do you have regarding collaboration with community medical professionals, including child psychiatrists?
(6) Is there a role for regional or statewide collaboration in ensuring access to medical and psychiatric expertise for ICC?
Yes. I think that is inherent in the responses lists above.
The medical and psychiatric needs of the members of the Rosie D. class are likely to vary from case to case; most children with Serious Emotional Disturbance will need a primary care provider and some sort of specialist in diagnostic evaluation and treatment (child psychiatrist, child neurologist or developmental/behavioral pediatrician). However, I would not separate them from the rest of the team- the physicians need to be tightly integrated with the team, not just consultants who intermittently offer opinions. One of the problems with the current model of "medication consultation" is that the psychiatrist is not afforded time to understand the patient and family before being forced to offer an opinion. Medical and psychiatrists serve several roles on the team:
1) Diagnostic: Sorting out these symptoms requires a physician who understands child development, the wide range of normal, and the various diagnoses we need to consider. They also are key to understanding the role of social factors and physical illness in the process.
2) Therapeutic: Physicians (generalist and specialist) often have a better idea of what is possible in the mileau in which the patient lives. They are also able to prescribe medications, although one must be careful of over-medicating or "off-label" use of medications.
3) Monitoring: Efficacy and side -effects. This approach has been well addressed in the "chronic disease model mentioned earlier.
4) Advocacy: A doctor can be of great assistance to the family in navigating the system.
A few ideas, which depend on the model of care:
1) If the CSAs serve mostly to link families and services through care coordination, then is incumbent on the CSAs to make connections with local resources. In areas that are currently devoid of services, the CSA may need to be the conduit for care.
2) In areas with little access to needed services, the MCPAP program can serve to support primary care physicians who often serve the role that would be better served by child psychiatrists.
3) CSAs in areas with few resources may wish to pursue telepsychiatry as a means of access for child psychiatry.
4) Supporting the expansion of the profession: All three of the subspecialists mentioned above are not well compensated for caring for these complex children. That needs to be addressed.
(2) Which of the needs listed above are likely to occur most often, or require most extensive use of medical or psychiatric expertise?
It seems to be that the hardest thing in all of this is the diagnostic formulation; in the ideal world that takes the most time, and requires clear thinking and a comprehensive overview of what is going on. Over and over again, we hear from families that "no one has truly evaluated my child", while the child is on a regime of 4 or 5 psychotropic medications, each one treating the side effects of the medication prescribed previously. The diagnosis in children has to be developmental and fluid, but as important is that the diagnostic process allow that family to be heard.
After that is the sorting of therapeutic options: medications (mostly prescribed off-label, with limited evidence), various forms of therapy, educational planning. In the new model, there will need to be an integration of things with the wraparound components.
(3) Based on your program experience and knowledge of the clinical workforce issues in your region of Massachusetts, what staffing arrangements make most sense for CSAs in providing medical and psychiatric expertise? Which disciplines (e.g., child psychiatrist, child-trained APRN, child-trained RN, behavioral pediatrician, or other medical professionals) can be most useful in which roles?
In Central Massachusetts, we have a strong group of primary care pediatricians who are interested and willing to work with children with SED, but who are beginning to feel the time pressure of practice- i.e. how do I make time in the day to be part of a multi-disciplinary team. We have a number of agencies working with children with mental health issues in Worcester and a robust private practice community in the Worcester city; psychiatric resources outside of the city are almost non-existent, especially in the South Central and Blackstone Valley regions. We have no access to behavioral pediatrics for children under 5 and one behavioral pediatrician for children over 5 IN THE ENTIRE COUNTY! Child psychiatry is a bit better- there are limited services for children in Worcester through 5 or 6 or so FTE child psychiatrists in the City, and 1.5 FTE in South Worcester County. Child neurology is similarly limited. The MCPAP program is robust, but is asked to see complex children frequently (given the conditions mentioned about)
(4) What suggestions/lessons learned do you have regarding collaboration with community medical professionals, including child psychiatrists?
1) Enable multiple modes of communication (beeper, phone, e-mail)
2) Allow short term consultation
3) Recognize the limits of the model.
The MCPAP has shown that the most important component of providing collaborative care is the development of an on-going relationship between the PCPs and the child psychiatrist; both professions can provide better care from the ability to converse in person and via e-mail. The program has allowed us to "leverage" existing resources in the County, which has been useful for both the SED kids and the kids who are "one notch below" SED. THe relationship must include a recognition by the consultant that, in most cases, when the PCP asks the consultant to meet with the family in person, that is a serious request that must be honored. Also, there are some kids where the MCPAP relationship is not enough- the system should have flexibility to allow psychiatry to move from a consultative to a therapeutic role, and back again.
(5) What are pros and cons of the CSA providing ongoing psychopharmacology services for enrolled children?
Given the overall shortage of providers for psychopharm services in the Commonwealth, it is difficult to think of any downside to the CSA providing services to clients. Except this: perhaps our shortage of providers is the only thing preventing a higher degree of overmedication than what we see already. The evidence base for much of our management of children with mental illness is small, and needs to grow. I would submit that any psychopharm services provided through the newly established CSA include a strong evaluation components, recognizing the quasi-experimental nature of much of this and serving as an entry point to a multitude of clinical trials designed to answer the question- is this medication in this situation worth the risk? The downside of providing more psychopharmacology is that the market will drive us to overmedicate, if we let it do so.
(6) Is there a role for regional or statewide collaboration in ensuring access to medical and psychiatric expertise for ICC?
Saturday, March 22, 2008
Guest Spot: Why I support changes in the Rosie D. case
Dear Health and Human Services:
I support new reforms for the children's mental health in the Commonwealth. The system is broken on how mental health services are delivered and paid for. It was only a matter of time until a lawsuit was filed by parents to advocate for improved mental health services for their children known as the Rosie D vs Romney case. As an independent advocate and mental health professional, I was appalled how parents had to take their kids to the local emergency rooms to get evaluated for mental health services when in fact some of the services that did not involve immediate medical treatments ( for example, life threatening situations) and stablization could have been done at outpatient clinics.
I support more intensive care management and family stabilization services to be conducted on the outpatient level and be in place from six months to a year for some families that are in danger of having their children taken away. Staff needs to be trained on how to interact and to counsel children who are dual diagnosed with psychiatric and physical disabilities.
I further advocate that parents be held accountable for some of their children's mental health issues. It is found after some investigations by the Department of Social Services that parents have their own mental health issues that need immediate attention. I don't understand why these parents are not pre-screened by their doctors before the leave the hospitals with their babies. The system is reactive, and after the fact, as damage is done to these children. Possibly a proactive measure would be to implement pre-screening tools for pregnant mothers and fathers to determine if they are capable of taking care of their children's phyiscal and mental health needs. If adoptive parents have to go through the same measures, then these parents need to go through the same thing as well.
Regarding the infrastructure, the mechanisms to pay providers, particularly social workers and mental health counselors are unfair and inequitable. There are some counselors across the state who are making the same money as their clients on SSI with children. It is demoralizing to hear my colleagues vent about they are not paid for no-shows and how difficult it is to make a sustainable living with a masters degree and/or advanced degree in their field. It is utmost important that the commonwealth change the way they pay mental health clinicians for their work. It is agreed as a consensus that there is a shortage of qualified mental health clinicians, and changing the infrastructure and values on how clinicians are paid for their work will decrease the shortage and children with mental health needs will be served.
Robbin Miller
Advocate/Counselor
I support new reforms for the children's mental health in the Commonwealth. The system is broken on how mental health services are delivered and paid for. It was only a matter of time until a lawsuit was filed by parents to advocate for improved mental health services for their children known as the Rosie D vs Romney case. As an independent advocate and mental health professional, I was appalled how parents had to take their kids to the local emergency rooms to get evaluated for mental health services when in fact some of the services that did not involve immediate medical treatments ( for example, life threatening situations) and stablization could have been done at outpatient clinics.
I support more intensive care management and family stabilization services to be conducted on the outpatient level and be in place from six months to a year for some families that are in danger of having their children taken away. Staff needs to be trained on how to interact and to counsel children who are dual diagnosed with psychiatric and physical disabilities.
I further advocate that parents be held accountable for some of their children's mental health issues. It is found after some investigations by the Department of Social Services that parents have their own mental health issues that need immediate attention. I don't understand why these parents are not pre-screened by their doctors before the leave the hospitals with their babies. The system is reactive, and after the fact, as damage is done to these children. Possibly a proactive measure would be to implement pre-screening tools for pregnant mothers and fathers to determine if they are capable of taking care of their children's phyiscal and mental health needs. If adoptive parents have to go through the same measures, then these parents need to go through the same thing as well.
Regarding the infrastructure, the mechanisms to pay providers, particularly social workers and mental health counselors are unfair and inequitable. There are some counselors across the state who are making the same money as their clients on SSI with children. It is demoralizing to hear my colleagues vent about they are not paid for no-shows and how difficult it is to make a sustainable living with a masters degree and/or advanced degree in their field. It is utmost important that the commonwealth change the way they pay mental health clinicians for their work. It is agreed as a consensus that there is a shortage of qualified mental health clinicians, and changing the infrastructure and values on how clinicians are paid for their work will decrease the shortage and children with mental health needs will be served.
Robbin Miller
Advocate/Counselor
Friday, March 21, 2008
View from the Front Lines: Trying to answer the questions.
Yesterday was another day where everyone had multiple agendas, and complicated problems. Not that I mind complicated problems (they are often the most interesting ones), but dealing with them preclude doing much work on these many questions from EOHHS. We should look at the next set. I'm going to tackle the last question first, but ultimately will fill in the blanks.
Clearly we will need to play with this, but I think that the work on care coordination done as part of the Medical Home initiative should have some impact. Care coordination for "children with special health care needs" can be classified by the coordinator on a three or four point scale, based on the needs of the child and family, and that "level" of CoC should guide the caseload. At a guess, I would think that a single coordinator could handle about 30 units of care per week, where level 1 is one unit, level 2 is 2 units, level 3 is 4 units and level 4 is 6 units, where a level 1 is a kid who is on maintainance/ check in once a week' mode, and level 4 is FST level- this family is about to implode. In an ideal world, the ICC would have some paraprofessionals so that the ICC could deploy different components of the team as needed.
Section 2.3A
(1) What staffing models would you recommend for ICC programs to enable them to serve children and youth and their families with diverse types of needs, needs that vary over time, and diverse levels of need? How could programs reliably respond to high levels of need in some families while simultaneously reliably serving families with less intense or acute needs?Clearly we will need to play with this, but I think that the work on care coordination done as part of the Medical Home initiative should have some impact. Care coordination for "children with special health care needs" can be classified by the coordinator on a three or four point scale, based on the needs of the child and family, and that "level" of CoC should guide the caseload. At a guess, I would think that a single coordinator could handle about 30 units of care per week, where level 1 is one unit, level 2 is 2 units, level 3 is 4 units and level 4 is 6 units, where a level 1 is a kid who is on maintainance/ check in once a week' mode, and level 4 is FST level- this family is about to implode. In an ideal world, the ICC would have some paraprofessionals so that the ICC could deploy different components of the team as needed.
(2) What staffing models would you recommend for families in which more than one Medicaid-eligible child needs ICC? The ICCs are going to need to build relationships with the families, and it makes sense to make things happen. Efficiency would dictate that weallow the kids in a family to have a single care provider.
(3) What do you recommend as qualifications for the ICC Care Manager? For supervisors?
(3) What do you recommend as qualifications for the ICC Care Manager? For supervisors?
ICC Care managers should be MSWs or really good BSW, or RNs with psych experiences, with experience in family centered care.
(4) What supervisory ratios, if any, would you suggest for both Care Managers and Family Mentors? Why? 1:6, given the level support these folks are facing. It is tough to tell you why, but that seems an appropriate number. What do the rest of you think?
(5) How would you recommend using Family Mentors, given the likely shortage of trained Family Mentors? Peculiar question; if we don't have them, how can we use them?
(6) What are the advantages and disadvantages of standardizing program staffing models? Of allowing the program staffing model to vary by ICC provider? This feels to me to be the most important question; Massachusetts and even Worcester County is not a uniform place, and what works in Boston may not work in Worcester (and what works in Worcester may not work in the rest of Worcester County). Programs should be judged by the results, not the means by which they get there. Anything short of that will simply not work.
(4) What supervisory ratios, if any, would you suggest for both Care Managers and Family Mentors? Why? 1:6, given the level support these folks are facing. It is tough to tell you why, but that seems an appropriate number. What do the rest of you think?
(5) How would you recommend using Family Mentors, given the likely shortage of trained Family Mentors? Peculiar question; if we don't have them, how can we use them?
(6) What are the advantages and disadvantages of standardizing program staffing models? Of allowing the program staffing model to vary by ICC provider? This feels to me to be the most important question; Massachusetts and even Worcester County is not a uniform place, and what works in Boston may not work in Worcester (and what works in Worcester may not work in the rest of Worcester County). Programs should be judged by the results, not the means by which they get there. Anything short of that will simply not work.
That said, evaluating the results of different staffing models is more difficult than ensuring program fidelity. Needs more input from the evaluaton team to disign appropriate measures.
Wednesday, March 19, 2008
Money makes the mental health integrate....
From the Maternal and Child Health E-Newsletter:
3. FUNDERS DISCUSS EFFORTS TO INTEGRATE MENTAL HEALTH AND ORAL HEALTH
INTO CHILDREN'S HEALTH CARE
Critical Services for Our Children: Integrating Mental and Oral Health into Primary Care presents a summary of a discussion among grantmakers and health services researchers about improving the children's health care system by better integrating oral and mental health services into primary care. The issue brief is based on a Grantmakers in Health Issue
Dialogue held on April 17, 2007, that focused on strategies for reducing fragmentation of services and explored opportunities for health funders. An overview of the issue, possible solutions, a conclusion, and references are provided. Topics include challenges to an integrated children's health system and examples of how health funders are addressing the problems. The issue brief is available here. An executive summary is also available here.
3. FUNDERS DISCUSS EFFORTS TO INTEGRATE MENTAL HEALTH AND ORAL HEALTH
INTO CHILDREN'S HEALTH CARE
Critical Services for Our Children: Integrating Mental and Oral Health into Primary Care presents a summary of a discussion among grantmakers and health services researchers about improving the children's health care system by better integrating oral and mental health services into primary care. The issue brief is based on a Grantmakers in Health Issue
Dialogue held on April 17, 2007, that focused on strategies for reducing fragmentation of services and explored opportunities for health funders. An overview of the issue, possible solutions, a conclusion, and references are provided. Topics include challenges to an integrated children's health system and examples of how health funders are addressing the problems. The issue brief is available here. An executive summary is also available here.
Tuesday, March 18, 2008
Responding to the RFI- Part 2
The CSA's are an interesting component of the proposed Rose D remedy; they have some questions about them as well:
 1. Do you have any comments or suggestions about the number or configuration of Service Areas?
1. Do you have any comments or suggestions about the number or configuration of Service Areas?
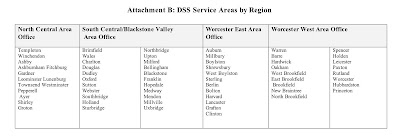
Combining South Central Worcester County and the Blackstone Valley is a mistake; the distance from Wales to Bellingham is about 40 miles, over 2 lane roads, without public transportation. The large area includes 3 community hospitals, one of which is quite small, and only one local agency capable of performing the tasks requested in the settlement. Several aspects of service delivery, including rapid response team and home based therapy, will be very difficult to deliver over such a wide service area. We would recommend that the CSA be split into two separate regions.
2. Do you have any comments or suggestions about the proposed scope of CSA services?
The scope of services for the CSA is a little confusing; by specifying that the services be provided by an subcontractor, but delivered within the MCE (and subject to review by the MCE), it seems to me that you are setting up barrier to care. The CSA really needs to be empowered to authorize levels of service for this to work quickly, at least within MassHealth. For example:
A new patient (Rosie C) is found eligible for services for bipolar disorder. Her mental health provider MCE-A refers her to their subcontractor CSA-A, who works with the family and determines that her needs include family and individual therapy, therapeutic day-school, respite care and psychopharm services. The CSA-A sends this plan to the MCE-A for review, and convenes the team meeting. The school disagrees with their part of the plan, DMH has trouble with the respite portion of the plan, noone can find a child psychiatrist in plan and all beg the pediatrician to keep prescribing the meds while they sort this all out. The CSA-A then asks the MCE-A to go out of plan to find a psychopharmocologist. After 2 months of meetings, none of the needed services are authorized or running.
Unfortunately, the CSA can't have control over DMH or DOE resources; the least we can do is give them some authority over the MassHealth portion of the package. Otherwise, we are are just adding another layer of bureaucracy.
 1. Do you have any comments or suggestions about the number or configuration of Service Areas?
1. Do you have any comments or suggestions about the number or configuration of Service Areas?Combining South Central Worcester County and the Blackstone Valley is a mistake; the distance from Wales to Bellingham is about 40 miles, over 2 lane roads, without public transportation. The large area includes 3 community hospitals, one of which is quite small, and only one local agency capable of performing the tasks requested in the settlement. Several aspects of service delivery, including rapid response team and home based therapy, will be very difficult to deliver over such a wide service area. We would recommend that the CSA be split into two separate regions.
2. Do you have any comments or suggestions about the proposed scope of CSA services?
The scope of services for the CSA is a little confusing; by specifying that the services be provided by an subcontractor, but delivered within the MCE (and subject to review by the MCE), it seems to me that you are setting up barrier to care. The CSA really needs to be empowered to authorize levels of service for this to work quickly, at least within MassHealth. For example:
A new patient (Rosie C) is found eligible for services for bipolar disorder. Her mental health provider MCE-A refers her to their subcontractor CSA-A, who works with the family and determines that her needs include family and individual therapy, therapeutic day-school, respite care and psychopharm services. The CSA-A sends this plan to the MCE-A for review, and convenes the team meeting. The school disagrees with their part of the plan, DMH has trouble with the respite portion of the plan, noone can find a child psychiatrist in plan and all beg the pediatrician to keep prescribing the meds while they sort this all out. The CSA-A then asks the MCE-A to go out of plan to find a psychopharmocologist. After 2 months of meetings, none of the needed services are authorized or running.
Unfortunately, the CSA can't have control over DMH or DOE resources; the least we can do is give them some authority over the MassHealth portion of the package. Otherwise, we are are just adding another layer of bureaucracy.
Monday, March 17, 2008
Responding to the RFI: What can the Commonwealth actually do?
So, here we are, moving into spring, and Children's Behavioral, Mental and Developmental Health in the Commonwealth is not yet fixed. What is wrong with us? As I mentioned in an earlier post, the Executive Office of the Health and Human Services (EOHHS) has offer us the opportunity to give them advice on how to fix a system that often seems clunky and unresponsive (and certainly seemed so to Judge Posner, in his recent ruling). Now is the time, it seems, to step up the plate, and let our opinions be know.
The Request for Information (which is still available on-line) has 68 specific questions, which have been carefully and thoughtfully written out for our review. We have until April 1 to give them a reply. After a few meetings with my colleagues in the Worcester Mental Health Network, I have been tasked with trying to formulate a reply that speaks to some of the unique characteristics of Central Massachusetts. They clearly have more confidence in my ability to do this than I do. On the other hand, it is our shot at getting some input into the process. So, I 'll give it a go.
First off, it is clear that the suggestions my Advocate Miller earlier in the blog are not terribly helpful. She has said on several occassions that the answer is to pay clinicians for no shows. The problem with that is that it encourages clincians to encourage no shows, to maximize revenue and minimize work. Bad idea, setting up a system ripe for abuse. As we move through the questions posed by MassHealth, I hope that we are able to help to create a system that is equitable, efficient and unlikely to engender fraud.
Let's look at the first set of questions:
(1) How would you recommend that MassHealth ensure that children and youth receive comprehensive assessments culminating in the completion of the Massachusetts CANS, at the times and places described above?
This is an interesting question. The CANS seems to be "a tool developed to assist in the management and planning of services to children and adolescents and their families with the primary objectives of permanency, safety, and improved quality in of life." which is used to assess the severity of a clinical problem, the impact on function, and the strengths that the child and family bring themselves to the table. It is not a functional status measure, yet many of us have concern that it will be used by agencies INSTEAD of the normed functional status measures that others are using.
The CANS assessments should be used as part of the diagnosis of psychiatric disorder, but as a means of determining whether or not the illness meets the threshold for a serious emotional disturbance. It should NOT replace the other functional status indicators such as the BASQ or the TOPS that are used in several of the "carve out" programs. Instead, the CANS should used sparingly, in order to document the need for a change in the level of care provided. Operationalizing this will be tricky, as the level of severity of mental illness can easily change over the course of a few days, but we wouldn't want to be repeating the CANS that frequently. The tool looks at performance over the past 30 days, and takes 2-4 hours to administer.
We are very troubled by one sentence in the RFI: "As a result, multiple clinicians may complete a Massachusetts CANS assessment for the same child within a short period of time. " Our concern is that will result in duplication of effort, focusing on lots of assessment and reassessment to the exclusion of treatment, and strongly urge the Commonwealth to allow multiple clinicians to work off of a single CANS assessment, especially if the number of clinicians able to perform the CANS is limited by the certification process.
Assuring access will require MassHealth to work with clinicians to develop criteria for the use of instrument, one of which should be parental desire for a more complete assessment.
(2) How would you recommend that MassHealth promote communication among multiple clinicians involved with the care of a child within the constraints of privacy and security laws?
Communication within a treatment team is paramount; the key to coordinating the flow of information has to be collaborative between the Intensive Care Coordinator and the parent; the parent needs to give or withhold consent, and the ICC has to have a handle on the flow of information. Many agencies have segregated information regarding mental health from the medical record of physicial health. This would be a mistake for these families- access to the full record is of the utmost importance.
To treat patients with SED requires free flow of information within the team. In developing the treatment plan, the ICC will need input from the clinician, the psychiatrist, the PCC and the school, as least in most cases. Add DMR, DYS, probation, and the court in another. The family, working with the ICC, will need to manage a complex data system, one that, in most cases will allow the various parties to speak to each other in a timely fashion. This can be done within the Virtual Gateway, a clinic based EMR or frequent phone calls. The first two options require the support of a new level of computing skills within the program. So, we are talking about an new and intimate relationship (family - ICC) that enables the members of the team to access some kind of "common record" that allows the family intimate contol over who sees what in this context. Ultimately, that probably needs to be an incredibly secure on-line resource or "vault" with different "windows" that allow families to specify what level of information one is permitted to see. One of the roles of the ICC would be to help families to ascertain who in the treatment team gets to see what part of the record.
(3) How would you recommend that MassHealth ensure coordination among clinicians assessing a child and not create the need for multiple assessments and reassessments?
Bingo. You have put your finger on the heart of the problem. How do you avoid multiple assessments, when your patients are tired of their problems and the creaky system. Early on in the process, MassHealth must encourage ALL parts of the treatment team to talk to each other, either by video conference or in person, and including at least the family (and the child, if the child is deemed sufficiently mature. The team needs to discuss what is known about the child at this time, create a plan for intervention and further evaluation and generate a timetable for review and reassessment (sorry, but review and reassessment are essential because kids grow up and change as they grow). MassHealth's tools:
The Request for Information (which is still available on-line) has 68 specific questions, which have been carefully and thoughtfully written out for our review. We have until April 1 to give them a reply. After a few meetings with my colleagues in the Worcester Mental Health Network, I have been tasked with trying to formulate a reply that speaks to some of the unique characteristics of Central Massachusetts. They clearly have more confidence in my ability to do this than I do. On the other hand, it is our shot at getting some input into the process. So, I 'll give it a go.
First off, it is clear that the suggestions my Advocate Miller earlier in the blog are not terribly helpful. She has said on several occassions that the answer is to pay clinicians for no shows. The problem with that is that it encourages clincians to encourage no shows, to maximize revenue and minimize work. Bad idea, setting up a system ripe for abuse. As we move through the questions posed by MassHealth, I hope that we are able to help to create a system that is equitable, efficient and unlikely to engender fraud.
Let's look at the first set of questions:
(1) How would you recommend that MassHealth ensure that children and youth receive comprehensive assessments culminating in the completion of the Massachusetts CANS, at the times and places described above?
This is an interesting question. The CANS seems to be "a tool developed to assist in the management and planning of services to children and adolescents and their families with the primary objectives of permanency, safety, and improved quality in of life." which is used to assess the severity of a clinical problem, the impact on function, and the strengths that the child and family bring themselves to the table. It is not a functional status measure, yet many of us have concern that it will be used by agencies INSTEAD of the normed functional status measures that others are using.
The CANS assessments should be used as part of the diagnosis of psychiatric disorder, but as a means of determining whether or not the illness meets the threshold for a serious emotional disturbance. It should NOT replace the other functional status indicators such as the BASQ or the TOPS that are used in several of the "carve out" programs. Instead, the CANS should used sparingly, in order to document the need for a change in the level of care provided. Operationalizing this will be tricky, as the level of severity of mental illness can easily change over the course of a few days, but we wouldn't want to be repeating the CANS that frequently. The tool looks at performance over the past 30 days, and takes 2-4 hours to administer.
We are very troubled by one sentence in the RFI: "As a result, multiple clinicians may complete a Massachusetts CANS assessment for the same child within a short period of time. " Our concern is that will result in duplication of effort, focusing on lots of assessment and reassessment to the exclusion of treatment, and strongly urge the Commonwealth to allow multiple clinicians to work off of a single CANS assessment, especially if the number of clinicians able to perform the CANS is limited by the certification process.
Assuring access will require MassHealth to work with clinicians to develop criteria for the use of instrument, one of which should be parental desire for a more complete assessment.
(2) How would you recommend that MassHealth promote communication among multiple clinicians involved with the care of a child within the constraints of privacy and security laws?
Communication within a treatment team is paramount; the key to coordinating the flow of information has to be collaborative between the Intensive Care Coordinator and the parent; the parent needs to give or withhold consent, and the ICC has to have a handle on the flow of information. Many agencies have segregated information regarding mental health from the medical record of physicial health. This would be a mistake for these families- access to the full record is of the utmost importance.
To treat patients with SED requires free flow of information within the team. In developing the treatment plan, the ICC will need input from the clinician, the psychiatrist, the PCC and the school, as least in most cases. Add DMR, DYS, probation, and the court in another. The family, working with the ICC, will need to manage a complex data system, one that, in most cases will allow the various parties to speak to each other in a timely fashion. This can be done within the Virtual Gateway, a clinic based EMR or frequent phone calls. The first two options require the support of a new level of computing skills within the program. So, we are talking about an new and intimate relationship (family - ICC) that enables the members of the team to access some kind of "common record" that allows the family intimate contol over who sees what in this context. Ultimately, that probably needs to be an incredibly secure on-line resource or "vault" with different "windows" that allow families to specify what level of information one is permitted to see. One of the roles of the ICC would be to help families to ascertain who in the treatment team gets to see what part of the record.
(3) How would you recommend that MassHealth ensure coordination among clinicians assessing a child and not create the need for multiple assessments and reassessments?
Bingo. You have put your finger on the heart of the problem. How do you avoid multiple assessments, when your patients are tired of their problems and the creaky system. Early on in the process, MassHealth must encourage ALL parts of the treatment team to talk to each other, either by video conference or in person, and including at least the family (and the child, if the child is deemed sufficiently mature. The team needs to discuss what is known about the child at this time, create a plan for intervention and further evaluation and generate a timetable for review and reassessment (sorry, but review and reassessment are essential because kids grow up and change as they grow). MassHealth's tools:
1) Higher rate of reimbursement for subsequent visits to those who show up to the meeting.
2) Creation of a network of "meeting centers" that allow distant clinicians to be present in a virtual meeting.
3) Major support for transportation for families to attend these sessions.
(4) What are the advantages and disadvantages of using an exclusively web-based CANS?
(4) What are the advantages and disadvantages of using an exclusively web-based CANS?
The big advantage that I see is that it would allow the CANS to be used collaboratively among the different providers, eliminating the need for repeated assessments by different agencies of the same tool. The downside is that it requires access to the web, a problem particularly while doing home-based work.
(5) What are the advantages and disadvantages of using the Virtual Gateway to access the CANS application? This one I need to take a "pass"on- if others in the network have thoughts, please leave them here. I have no personal experience in using the Virtual Gateway.
(6) If you are a provider, do you currently have internet access? Most of the agencies in the Worcester Mental Health Network have internet access. That said, we have not yet figured out how to use that access forsecure communication with patients or each other yet. State support in this effort would be useful.
(5) What are the advantages and disadvantages of using the Virtual Gateway to access the CANS application? This one I need to take a "pass"on- if others in the network have thoughts, please leave them here. I have no personal experience in using the Virtual Gateway.
(6) If you are a provider, do you currently have internet access? Most of the agencies in the Worcester Mental Health Network have internet access. That said, we have not yet figured out how to use that access forsecure communication with patients or each other yet. State support in this effort would be useful.
Friday, March 14, 2008
Also of Interest: My e-mail runneth over...
Still off running a conference: I promise more substantive blogging soon. But this came from an Academy Listserve that I am on, and seemed worth sharing:
Paper Highlights State and Local Innovation in Finance Policy for Child Behavioral Health Services
from MCH Alert, March 7, 2008
Towards Better Behavioral Health for Children, Youth and Their Families: Financing That Supports Knowledge provides an overview of sources of funding (and their policy roots) that underwrite children's behavioral health services, illuminating the flaws and prospects of various policy choices. The working paper is the third in a series titled Unclaimed Children Revisited produced by the National Center for Children in Poverty. Although the paper focuses on public funding for mental health and on substance abuse services within the behavioral health arena, it also addresses related funding in education, child welfare, and juvenile justice. Topics include an overview of children's behavioral services, an overview of federal behavioral health funding streams and their impact, fiscal innovation in states and local communities, and challenges and opportunities. The authors conclude the paper with recommendations for policy actions to create and sustain a supportive federal and state fiscal environment. The paper is available here.
from MCH Alert, March 7, 2008
Towards Better Behavioral Health for Children, Youth and Their Families: Financing That Supports Knowledge provides an overview of sources of funding (and their policy roots) that underwrite children's behavioral health services, illuminating the flaws and prospects of various policy choices. The working paper is the third in a series titled Unclaimed Children Revisited produced by the National Center for Children in Poverty. Although the paper focuses on public funding for mental health and on substance abuse services within the behavioral health arena, it also addresses related funding in education, child welfare, and juvenile justice. Topics include an overview of children's behavioral services, an overview of federal behavioral health funding streams and their impact, fiscal innovation in states and local communities, and challenges and opportunities. The authors conclude the paper with recommendations for policy actions to create and sustain a supportive federal and state fiscal environment. The paper is available here.
Back to the frozen north soon!
Thursday, March 13, 2008
Screening in Month 3: How's it going?
This came across my e-mail today, and seemed relevant:
"3. MANUAL PROVIDES GUIDANCE IN CHOOSING PEDIATRIC DEVELOPMENTAL SCREENING INSTRUMENTS: Pediatric Developmental Screening: Understanding and Selecting Screening Instruments informs practitioners' selection and application of screening instruments in a range of practice settings. The Web-based manual, developed by the Commonwealth Fund, is based on a review of the scientific research on available developmental screening instruments. Part 1 is designed to facilitate the selection of screening instruments by helping practitioners define their practice needs. Part 2 presents guides designed to facilitate practitioners' abilities to compare developmental screening instruments with respect to clinical utility in practice settings and validity, or sensitivity and specificity, in
different populations and at various ages. An interactive Web feature (flow chart) is also available to answer questions about screening needs and make instrument recommendations. The manual is available through the Commonwealth Fund"
"3. MANUAL PROVIDES GUIDANCE IN CHOOSING PEDIATRIC DEVELOPMENTAL SCREENING INSTRUMENTS: Pediatric Developmental Screening: Understanding and Selecting Screening Instruments informs practitioners' selection and application of screening instruments in a range of practice settings. The Web-based manual, developed by the Commonwealth Fund, is based on a review of the scientific research on available developmental screening instruments. Part 1 is designed to facilitate the selection of screening instruments by helping practitioners define their practice needs. Part 2 presents guides designed to facilitate practitioners' abilities to compare developmental screening instruments with respect to clinical utility in practice settings and validity, or sensitivity and specificity, in
different populations and at various ages. An interactive Web feature (flow chart) is also available to answer questions about screening needs and make instrument recommendations. The manual is available through the Commonwealth Fund"
Sat with a few providers the other day, pondering the current screening program and speculating about what to do next. Only a few glitches identified:
1) Screening kids under two years of age for behavioral problems makes no sense: The parents understand the need to screen development, but find the behavioral questions irrelevant, especially at two weeks of age. It would be better if Masshealth were to require fewer screens early in childhood for behavioral health problems, and let us focus on developmental issues at that time. Also, the major behavioral health issue that affects the behavioral health of 2 week olds is maternal depression; we need to be developing a system to deal with that.
2) Billing remains complex: Since most of us treat all of our patients the same, using the screening code and the modifiers has resulted in a some of our patients with "out of state" insurances getting billed for the screening, to their dismay. Makes me long for the days of a single payer system (wait, we haven't had those days yet).
3) U1 and U2 mean what?: We all have found that the PSC doesn't identify a number of kids that we think have fairly significant problems, some of which are on-going and some of which are new, and think that the "yes/no" coding is too simplistic (don't capture the richness of what is actually going on.
4) Teens and confidentiality: We've had a couple cases now where parents looked at their kids PSC before it was collected, and argued with their kid about his "self-report". Not sure that we have helped parent-child interaction in those cases.
Still, most folks were feeling pretty good about how things were going.
I'm running a meeting in a faraway place this week, which is why the postings have been sparse. More next week.
Wednesday, March 12, 2008
Rosie D. and US: implications for the “Medical Home”
Hello there, and thanks to David for letting me “blog” about this great topic. I’ve never “blogged” before (sounds like a trudge through a swamp), so here goes.
As you know, one great thing about the Rosie D. decision is that it mandates mental health screening for all children through their source of primary care. While this is great in that it identifies lots of kids who need mental health services and will hopefully make sure they are connected to those services, not much has been said about the ongoing parent-primary care-mental health provider partnership that such a system should create. For any of you new to the concept of the “medical home”, it has a long, drawn-out definition. However, in 25 words or less, its core is the partnership between parents, children and youth, and the child’s primary care practice as a center of coordination of care.
I’m co-leader with Dr. Rich Antonelli of the Central Massachusetts Medical Home Network Initiative (CMMHNI), a project to improve comprehensive, coordinated, continuous care for children and youth with special health care needs in a group of interested primary care pediatric practices (Medical Homes), and one of our major activities is to build and strengthen connections between Medical Homes and community-based service organizations. The Rosie D. decision represents a tremendous opportunity to strengthen coordination and collaboration between mental health service providers and primary care practices. We are committed to working toward ensuring that the recent court decision will be implemented in a way that benefits Medical Home-mental health service provider partnerships.
Working with our mental health partners in Central Mass. in our thoughts about responding to the recent RFI (Request for Input), we’ve come up with the following principles that, from our perspective, are critical for inclusion in the activities of the Rosie D. initiative as it moves forward:
- The need for bidirectional education between mental health service providers and Medical Homes about the needs of children and families under our care;
- The need for bidirectional discussion and idea sharing between mental health service providers and Medical Homes about how to best provide coordinated services to shared patients/clients and their families;
- The need for ongoing communication between mental health service providers and medical homes about mental health evaluation and services provided to children who are referred, to enable ongoing involvement of the medical home in care, high-quality coordination of these services with other health care and school-related services provided to the family, and more efficient care (including avoidance of duplication of care);
- The need for crisis plans and crisis teams to engage in communication and coordination with the child's ongoing medical and mental health service providers, as well as with their school. The goal of this process would be to help children and families transition smoothly between levels of care (both up and down the urgency/intensiveness ladder).
- The need for proactive designation of a person or small group of people as each child's crisis team, ideally determined BEFORE a crisis occurs. This would further enable well-planned, well-coordinated care.
In a nutshell, we are interested in planning for “what happens after the referral, to make sure children receive the highest-quality coordinated care?”
Thanks to Beth Pond, Barbara Donati, Rich Antonelli, Meri Viano, and Lisa Lambert for their help in putting this together. I’d be happy to hear any thoughts you might have about this. Feel free to contact me at stillec@ummhc.org, or post a reply. Thanks for your attention!
Chris Stille, MD, MPH
General Pediatrics, UMass
Co-Principal Investigator, CMMHNI
Wednesday, March 5, 2008
How a Bill becomes Law: Update on the Children’s Mental Health Campaign
I hate driving to Boston. Even with GPS, I get lost. And GPS doesn’t find you a parking place. Still, on the day after the Rhode Island Primary, I hopped in my care to drive into Boston to hear Mary Lou Sudders (head of MSPCC) and David DeMaso MD (head of psychiatry at Children’s) talk about the Children’s Mental Health Initiative, a bill currently winding it’s way through the Massachusetts’ legislature that complements all of the work that we are doing with the Rosie D. case. As we have said repeatedly on this blog, Rosie D. is a tremendous opportunity for change in the system for kids on MassHealth. This bill offers the opportunity to bring similar changes to the rest of the kids in Massachusetts.
So, with my car carefully parked in a quasi-legal space, I arrived late to a brilliant session on the current state of the legislation. “An Act Relative to Children’s Mental Health” was introduced into the Massachusetts legislature on 1/10/2007, and it is currently clearing the committee hurdles.
The bill is based on a premise: that there is (and shouldn’t be) a single system for mental health care, but that the key to the process is to be building bridges between the various folks who work with the kids who do the work. Partnerships, with Health Care for All, with the Parent Professional Advocacy League and Health Law Advocates, are the key to moving this process along. All of these agencies are key to this process. To emphasize the point, the two presenters alternated sentences in the presentation of the material. This partnership has led to co-sponsorship by 96 legislators, as the coalition educates the legislature on what this bill is about and assures them that this is the right thing for the legislature to do.
The bill is HB4276 and has five key elements. First, the bill creates a single voice within the government for children’s mental health, the Commissioner of Mental Health. (like the Commissioner of Public Health handles hospitals). This will be a major step in breaking down the silos. Second, the bill calls for payment of primary care doctors are paid for early screening in practice. Third, it provides for payment for the provision of collateral mental health services and collaboration. Fourth, it requires coordination of care within public agencies. There was a fifth thing, but I missed it by not typing fast enough.
The original bill also had some mental health parity law language that has been moved out of the omnibus bill into its own bill. Strategically, mental health parity is likely to need more pushing to get it through.
It has been quite a process moving the Omnibus Bill through the process. Its first committee was the Joint Committee on Mental Health and Substance Abuse. After a tremendous hearing, the bill was sent on to the Joint Committee on Health Care Finance, a committee that often doesn’t let bills out for consideration. The Bill was then sent to the Senate Ways and Means committee (in order to avoid the logjam in the House over the budget). In so doing, it was renamed; it is now called S.2518. When the bill makes it out of Senate Ways and Means, it needs to clear the House and to go to the Governor for signature. It is quite a process, and requires those of us on the ground to continue to support the bill to keep it moving through the process.
Children’s has been pushing this within the Children’s Hospital system. They have trained speakers, developed a website, sponsored a Mental Health Advocacy Day. MSPCC has been working with their advocacy network. So far, only two groups have come out against this: the Church of Scientology and the Mass Association of Health Plans. To make this work, they need our help. So what can we do?
1) Give voice to the stories: The folks in the State House need to hear the stories that are happening in different parts of the state. This is probably the single most important thing.
2) Get into the media: Op-Eds, letters to the editor, interviews; all of this is good. “The most important thing is not how well you are quoted, but how badly you are mis-quoted", to quote Ms. Sudders. While there is risk involved in talking to the media, there is benefit to getting this issue out and in the open. The media keeps the mission alive.
3) Talk to your legislators: They need to hear that this is their problem, not just a problem at Children’s.
Politically, the presenters thought that this was likely to be passed this year with the right support. A group of us are planning a series on events in Worcester County around mental health month to promote this initiative. Stay tuned for the details.
Oh, and if anyone wants to join the fight, give Matt Noyes (mnoyes@hcfama.org) a holler. He’ll hook you up.
So, with my car carefully parked in a quasi-legal space, I arrived late to a brilliant session on the current state of the legislation. “An Act Relative to Children’s Mental Health” was introduced into the Massachusetts legislature on 1/10/2007, and it is currently clearing the committee hurdles.
The bill is based on a premise: that there is (and shouldn’t be) a single system for mental health care, but that the key to the process is to be building bridges between the various folks who work with the kids who do the work. Partnerships, with Health Care for All, with the Parent Professional Advocacy League and Health Law Advocates, are the key to moving this process along. All of these agencies are key to this process. To emphasize the point, the two presenters alternated sentences in the presentation of the material. This partnership has led to co-sponsorship by 96 legislators, as the coalition educates the legislature on what this bill is about and assures them that this is the right thing for the legislature to do.
The bill is HB4276 and has five key elements. First, the bill creates a single voice within the government for children’s mental health, the Commissioner of Mental Health. (like the Commissioner of Public Health handles hospitals). This will be a major step in breaking down the silos. Second, the bill calls for payment of primary care doctors are paid for early screening in practice. Third, it provides for payment for the provision of collateral mental health services and collaboration. Fourth, it requires coordination of care within public agencies. There was a fifth thing, but I missed it by not typing fast enough.
The original bill also had some mental health parity law language that has been moved out of the omnibus bill into its own bill. Strategically, mental health parity is likely to need more pushing to get it through.
It has been quite a process moving the Omnibus Bill through the process. Its first committee was the Joint Committee on Mental Health and Substance Abuse. After a tremendous hearing, the bill was sent on to the Joint Committee on Health Care Finance, a committee that often doesn’t let bills out for consideration. The Bill was then sent to the Senate Ways and Means committee (in order to avoid the logjam in the House over the budget). In so doing, it was renamed; it is now called S.2518. When the bill makes it out of Senate Ways and Means, it needs to clear the House and to go to the Governor for signature. It is quite a process, and requires those of us on the ground to continue to support the bill to keep it moving through the process.
Children’s has been pushing this within the Children’s Hospital system. They have trained speakers, developed a website, sponsored a Mental Health Advocacy Day. MSPCC has been working with their advocacy network. So far, only two groups have come out against this: the Church of Scientology and the Mass Association of Health Plans. To make this work, they need our help. So what can we do?
1) Give voice to the stories: The folks in the State House need to hear the stories that are happening in different parts of the state. This is probably the single most important thing.
2) Get into the media: Op-Eds, letters to the editor, interviews; all of this is good. “The most important thing is not how well you are quoted, but how badly you are mis-quoted", to quote Ms. Sudders. While there is risk involved in talking to the media, there is benefit to getting this issue out and in the open. The media keeps the mission alive.
3) Talk to your legislators: They need to hear that this is their problem, not just a problem at Children’s.
Politically, the presenters thought that this was likely to be passed this year with the right support. A group of us are planning a series on events in Worcester County around mental health month to promote this initiative. Stay tuned for the details.
Oh, and if anyone wants to join the fight, give Matt Noyes (mnoyes@hcfama.org) a holler. He’ll hook you up.
Monday, March 3, 2008
Rosie D. and You: MassHealth wants your ideas!
MassHealth has issued a Request for Information on the Rosie D. case. It was posted on Friday afternoon, and you can get it here or by going to COM-PASS and searching all solicitation for “behavioral health”. It’s called Children's Behavioral Health Initiative RFI and it is quite long, but I think asks some good questions. As we discussed, last month, I think that it is important for us to formulate a response that speaks for the needs of children in Worcester County. (and for that matter, the rest of Massachusetts.) Responses are due by April 1.
In Worcester, the Network will be meeting to discuss our responses:
Monday, March 17, 4 PM, Bowditch and Dewey:
Central Mass Responds: A discussion of possible responses to the RFI by the membership of the Network.
Look for more updates on this blog.
In Worcester, the Network will be meeting to discuss our responses:
Monday, March 17, 4 PM, Bowditch and Dewey:
Central Mass Responds: A discussion of possible responses to the RFI by the membership of the Network.
Look for more updates on this blog.
Subscribe to:
Posts (Atom)

